Assistant Professor Icahn School of Medicine at Mount Sinai New York, New York
Disclosure(s):
Kris Foley, MD: No financial relationships to disclose
Case Diagnosis: Agitation in Anoxic Brain Injury
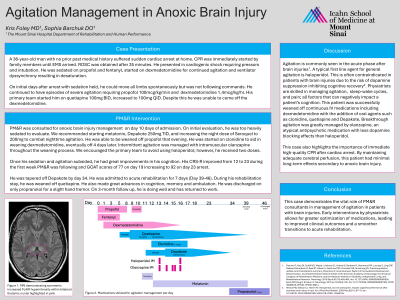
Case Description or Program Description: A 36-year-old man with no prior medical history suffered sudden cardiac arrest at home. ROSC was achieved after 35 minutes. He presented in cardiogenic shock, requiring pressors, intubation, and sedation with propofol, fentanyl, and Precedex for agitation and ventilator dyssynchrony leading to desaturation. Initially, with sedation held, he moved all limbs but did not follow commands. Severe agitation required propofol (100 mcg/kg/min), Precedex (1.4 mcg/kg/hr), Seroquel (100 mg q6h), and trazodone (25 mg nightly). PM&R was consulted for anoxic brain injury 10 days post-admission. On first evaluation, he was overly sedated. We recommended melatonin, Depakote (250 mg/250 mg/500 mg), and increasing Seroquel to 200 mg for nighttime agitation. Propofol was weaned that evening, and clonidine was started to aid Precedex weaning, which was off in four days. Intermittent agitation was managed with IM olanzapine. Though we recommended against haloperidol, he received two doses. With sedation and agitation controlled, cognition improved significantly. His CRS-R increased from 12 to 23 in one week under PM&R care, with GOAT scores of 77 and 92 on days 19 and 23 post-arrest. He was admitted to acute rehabilitation for seven days, successfully weaned off Depakote and Seroquel, and discharged on propranolol (for tremor) and trazodone. At three-month follow-up, he had returned to work.
Setting: Inpatient consults
Assessment/Results: A 36-year-old with uncontrolled agitation on a ventilator after cardiac arrest showed significant improvement with PM&R’s titration of oral medications, including Seroquel and Depakote.
Discussion (relevance): Agitation is common post-brain injury. Haloperidol, a first-line agent, can hinder cognitive recovery due to dopamine suppression. Physiatrists manage agitation, sleep-wake cycles, and pain—critical factors in cognition.
Conclusions: PM&R consultants play a crucial role in agitation management post-brain injury. Early intervention facilitates smoother transitions to rehabilitation and improves cognitive recovery.

.jpg)
 photo")
