Resident Physician Ohio State University Wexner Medical Center Columbus, Ohio
Disclosure(s):
Gregory CJ Moellering, MD: No financial relationships to disclose
Case Diagnosis: A 39 y/o male who presented to the PM&R Spasticity Clinic with five years of mid thoracic paraspinal pain and perceived neck flexion weakness was found to have cervical dystonia which improved with initial trigger point injections and, ultimately, neurotoxin injection into his mid-low thoracic trapezius muscles.
Case Description or Program Description: A 39 y/o male who was referred to spasticity clinic after being seen by various physicians over five years for posterior cervical and mid thoracic back pain and neck flexion weakness. His workup including head and spine imaging and ultrasound of cervical and thoracic musculature was unremarkable.
Setting: Outpatient Spasticity Clinic
Assessment/Results: Physical exam demonstrated denser and firmer muscle bulk of mid to low trapezius muscles on left side which were tender to palpation. His head positioning was in slight right lateral flexion and left lateral rotation with limited lateral neck flexion and rotation bilaterally, and he was noted to have neck flexion weakness that improved while prone.
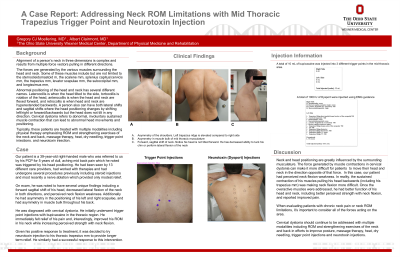
Initial trigger point injection of 10 cc of bupivicaine to mid-low thoracic area provided immediate, although temporary, relief of back pain and improved neck flexion. His subsequent visit included neurotoxin injection for longer relief.
Discussion (relevance): This case exemplifies the importance of muscle antagonism in cervical dystonia. His perceived neck flexion weakness likely was a result of a constant opposing force generated by dystonic trapezius muscles which his neck flexors, rather than being inherently weak, simply had difficulty overcoming. Additionally, pain secondary to the dystonia further limited his head movement. In these scenarios, trigger point injections with bupivicaine and/or neurotoxin to thoracic trapezius (not only cervical trapezius) could provide improvement of symptoms.
Conclusions: Trigger point injections and neurotoxin injections to mid to low thoracic trapezius muscles could provide symptomatic relief for select patients who have neck flexion limitations due to dystonia.

.jpg)