Resident, PGY-4 Ohio State University College of Medicine Columbus, Ohio
Disclosure(s):
Lara de Almeida, DO: No financial relationships to disclose
Case Diagnosis: Nodular Lymphocytic Myositis
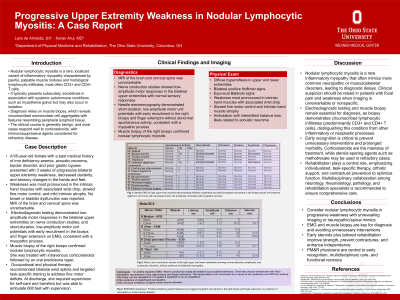
Case Description or Program Description: A 65-year-old female with past medical history of iron deficiency anemia, acoustic neuroma, bipolar disorder, and prior gastric bypass presented with three weeks of progressive bilateral upper extremity weakness, decreased dexterity, and sensory changes in her hands and feet. She was previously independent with activities of daily living and participated in Pilates. Examination revealed diffuse hyperreflexia, bilateral positive Hoffman signs, and equivocal Babinski signs. MRI of the brain and cervical spine was unremarkable. PM&R was consulted for electrodiagnostic evaluation. Nerve conduction studies (NCS) showed low-amplitude motor responses in the bilateral upper extremities. Needle electromyography (EMG) demonstrated short-duration, low-amplitude motor unit potentials with early recruitment in the right biceps and finger extensors, consistent with a myopathic process. No abnormal spontaneous activity was observed. Findings localized the weakness to a primary muscle disorder. Muscle biopsy of the right biceps confirmed nodular lymphocytic myositis. She received intravenous corticosteroids followed by an oral prednisone taper. Occupational and physical therapy identified slowed fine motor tasks due to wrist drop, intrinsic hand muscle atrophy, and MP flexion contractures. She required supervision for dressing, feeding, and grooming. Bilateral wrist splints were prescribed. She ambulated 600 feet with supervision but demonstrated intermittent balance loss, likely related to her acoustic neuroma.
Setting: Tertiary care hospital
Assessment/Results: At discharge from acute care, she required supervision for transfers and self-care with slight improvement in upper extremity function. Outpatient therapy and follow-up with Rheumatology and Neuromuscular clinic was arranged.
Discussion (relevance): This case highlights the rehabilitation challenges of nodular lymphocytic myositis, a rare inflammatory myopathy. Electrodiagnostic testing was essential for diagnosis when imaging was inconclusive. Orthotic use and task-specific training were critical in addressing upper extremity weakness and fine motor deficits.
Conclusions: Early electrodiagnostic evaluation and individualized rehabilitation, including orthotic support and task-specific therapy, are essential for improving outcomes in nodular lymphocytic myositis.

.jpg)