Resident University of Kansas Medical Center PM&R Program Overland Park, Kansas
Disclosure(s):
William Harrah, DO: No financial relationships to disclose
Case Diagnosis: This case highlights the complexity of recovery for patient's with HMGCR antibody-positive IMNM.
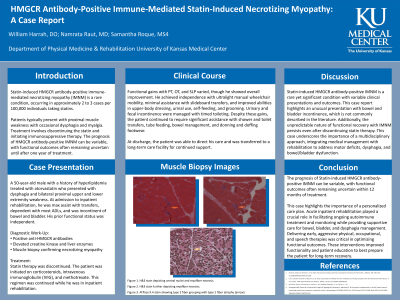
Case Description or Program Description: A 50-year-old male with a history of hyperlipidemia treated with atorvastatin presented with dysphagia and proximal weakness in all extremities. On admission to inpatient rehabilitation, he required maximal assistance for transfers, was dependent in most activities of daily living, and experienced bowel and bladder incontinence. Diagnostic work-up revealed positive anti-HMGCR antibodies, elevated creatine kinase and liver enzymes, and a muscle biopsy confirming necrotizing myopathy. Statin therapy was discontinued, and he was started on corticosteroids, intravenous immunoglobulin (IVIG), and methotrexate, which was continued throughout his inpatient rehabilitation stay.
Setting: Inpatient Rehab
Assessment/Results: Functional gains with PT, OT, and SLP varied, though he showed overall improvement. He achieved independence with ultralight manual wheelchair mobility, minimal assistance with slideboard transfers, and improved abilities in upper-body dressing, urinal use, self-feeding, and grooming. Urinary and fecal incontinence were managed with timed toileting. Despite these gains, the patient continued to require significant assistance with shower and toilet transfers, tube feeding, bowel management, and donning and doffing footwear.
Discussion (relevance): Statin-induced HMGCR antibody-positive IMNM is a rare yet significant condition with variable clinical presentations and outcomes. This case report highlights an unusual presentation with bowel and bladder incontinence, which is not commonly described in the literature. Additionally, the unpredictable nature of functional recovery with IMNM persists even after discontinuing statin therapy. This case underscores the importance of a multidisciplinary approach, integrating medical management with rehabilitation to address motor deficits, dysphagia, and bowel/bladder dysfunction.
Conclusions: The prognosis of this condition can be variable, with functional outcomes often remaining uncertain within 12 months of treatment. Acute inpatient rehabilitation played a crucial role in facilitating ongoing autoimmune treatment while providing supportive care for bowel, bladder, and dysphagia management. Delivering early, aggressive therapies werecritical in optimizing functional outcomes.

.jpg)