Assistant Professor Icahn School of Medicine at Mount Sinai New York, New York
Disclosure(s):
Kris Foley, MD: No financial relationships to disclose
Case Diagnosis: Uncontrolled Spasms Leading to Delayed Emergence from Anoxic Brain Injury
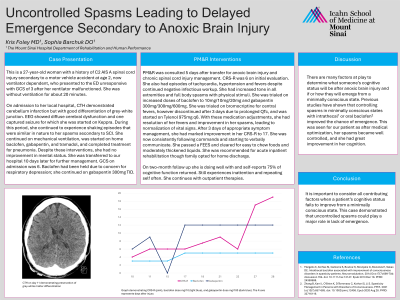
Case Description or Program Description: A 27-year-old C2 AIS-A woman (secondary to an MVA at age 2, now ventilator-dependent) presented to the ED unresponsive after a ventilator malfunction, resulting in ~20 minutes of apnea. On admission to a local hospital, CT head showed cerebellar infarction but preserved gray-white differentiation. EEG demonstrated diffuse cerebral dysfunction with one captured seizure. She was started on Keppra, however, exhibited persistent shaking resembling pre-existing SCI-related spasms. Despite mechanical ventilation, home baclofen, gabapentin, tramadol, and pneumonia treatment, her mental status did not improve. Ten days later, she was transferred to our hospital. Baclofen had been held due to respiratory concerns, and she remained on gabapentin 300mg TID. PM&R was consulted five days post-transfer for anoxic brain injury and chronic SCI management. Initial CRS-R was 6. She exhibited tachycardia, hypertension, fevers, increased tone, and full-body spasms with physical stimuli. Baclofen was resumed and titrated to 10mg/10mg/20mg, while gabapentin was increased to 300mg/300mg/600mg. Fevers were controlled with Tylenol 975 mg q6h. With symptom management, her fevers and spasms resolved, vital signs stabilized, and CRS-R improved to 17 within three days. She began following commands and verbally communicating. At two-month follow-up, she reported 75% cognitive recovery, with residual inattention and repetition.
Setting: Inpatient Consults
Assessment/Results: A 27-year-old C2 AIS-A patient who suffered anoxic brain injury had delayed emergence from a minimally conscious state (MCS) due to uncontrolled spasms.
Discussion (relevance): Cognitive recovery after anoxic brain injury is multifactorial. Studies suggest that controlling spasms with oral or intrathecal baclofen improves emergence. This was evident in our patient, whose cognition significantly improved once spasms were managed.
Conclusions: When cognitive recovery is delayed in a MCS uncontrolled spasms should be considered as a contributing factor. This case highlights the importance of optimizing spasticity management to facilitate emergence.

.jpg)
 photo")
