Associate Professor JFK Johnson Rehabilitation Institute Edison, New Jersey
Disclosure(s):
Ben Birkenfeld, MD: No financial relationships to disclose
Case Diagnosis: Neuropathic Pain after Acute Neuroinvasive West Nile Virus Infection
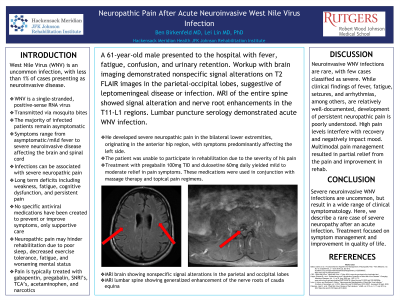
Case Description or Program Description: A 61-year-old male presented to the hospital with fever, fatigue, confusion, and urinary retention. Workup with brain imaging demonstrated nonspecific signal alterations on T2 FLAIR images in the parietal-occipital lobes, suggestive of leptomeningeal disease or infection. MRI of the entire spine showed signal alteration and nerve root enhancements in the T11-L1 regions. Lumbar puncture serology demonstrated acute West Nile Virus (WNV) infection. He received supportive treatment in the acute care hospital. Upon admission to inpatient rehabilitation, the patient demonstrated profound weakness and mental clouding. Interestingly, the patient developed severe neuropathic pain in the bilateral lower extremities, originating in the anterior hip region, with symptoms predominantly affecting the left side. The symptoms limited his ability to sleep at night and participate in rehabilitation activities during the day. The patient was started on neuropathic agents and required titration of pregabalin to 100mg TID and duloxetine to 60mg daily before starting to feel relief.
Setting: Acute Inpatient Rehabilitation
Assessment/Results: A patient with acute neuroinvasive WNV, demonstrated by signal abnormalities in the brain and spinal cord, presented to acute inpatient rehabilitation with overwhelming debilitation as well as severe lower extremity (left greater than right) neuropathic pain. Treatment with pregabalin 100mg three times daily and duloxetine 60mg daily helped with alleviation, enabling participation in rehabilitation therapies.
Discussion (relevance): Neuroinvasive WNV infections are rare, with an even smaller proportion deemed severe. While clinical findings of fever, fatigue, seizures, arrhythmias, among others, are relatively well-documented, development of persistent neuropathic pain is poorly understood. Multimodal pain management resulted in partial relief from the pain.
Conclusions: Severe neuroinvasive WNV infections are uncommon, but result in a wide range of clinical symptomatology. Here, we describe a rare case of severe neuropathy after an acute infection. Treatment focused on symptom management and improvement in quality of life.

.jpg)