Clinical Assistant Professor University of Iowa Health Care Iowa City, Iowa
Disclosure(s):
Brian Gu, Other: No financial relationships to disclose
Case Diagnosis: 79-year-old female with posterior reversible encephalopathy syndrome (PRES) in setting of Lyme neuroborreliosis.
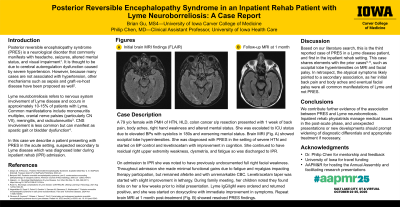
Case Description or Program Description: Patient presented to local hospital with new back pain, body aches, right hand weakness, and altered mental status. On hospital day 3, she developed aphasia and was no longer following commands. Brain MRI showed occipital lobe hyperintensities on multiple sequences, findings which were associated with severe hypertension. She was transferred to higher level of care and found to be rambling, disoriented, and aphasic. Neurology diagnosed PRES and started her on levetiracetam for seizure tendency on EEG. Over next several days, she showed some cognitive improvement but continued to have confusion, right upper extremity weakness, dysmetria, and fatigue. Therefore, she was discharged to an inpatient rehab facility (IRF).
Upon admission to IRF, she was found to have slight right full facial weakness not previously documented. She made minimal functional gains throughout admission primarily due to diffuse body aches and lethargy. Starting taper of levetiracetam improved performance slightly, but facial palsy, body aches and myalgias/arthralgias persisted. At family meeting 3 weeks into IRF admission, children noted they had found ticks on her a few weeks prior to initial presentation. Lyme IgM/IgG returned positive. She was started on doxycycline with rapid improvement in symptoms. Repeat brain MRI showed resolved PRES findings.
Setting: IRF associated with academic medical center.
Assessment/Results: At 2-3 month follow-ups, she endorsed complete resolution of symptoms, including facial palsy, right upper extremity strength, body aches and fatigue. She was walking independently and returned to driving.
Discussion (relevance): This is the third reported case, to our knowledge, of PRES associated with Lyme neuroborreliosis, and first in the inpatient rehab setting.
Conclusions: PRES should be considered as a potential complication of Lyme neuroborreliosis. Inpatient rehab providers manage medical issues in the post-acute phase, and unexpected developments should prompt consideration of new/previously undiagnosed conditions.

.jpg)
.jpg "Brian Gu, Other photo")
