Assistant Professor University of Utah PM&R Program Salt Lake City, Utah
Disclosure(s):
Daniella LaPlante, MD: No financial relationships to disclose
Case Diagnosis: Tinnitus after resection of pineal region glioblastoma.
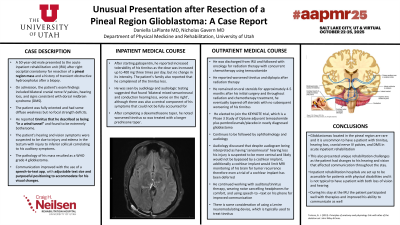
Case Description or Program Description: A 50-year-old male presented to the acute inpatient rehabilitation unit (IRU) after right occipital craniotomy for resection of a pineal region mass and a history of transient obstructive hydrocephalus after a biopsy. On admission, the patient’s exam findings included bilateral cranial nerve IV palsies, hearing loss, and signs consistent with dorsal midbrain syndrome (DMS). The patient was fully oriented and had some diffuse weakness but no focal strength deficits. At that time, he also reported tinnitus that he found to be bothersome and described as being “in a wind tunnel.” The pathology of his mass resulted as a WHO grade 4 glioblastoma. During his stay at the IRU the patient participated well with therapies.
Setting: Inpatient Rehabilitation.
Assessment/Results: The patient’s hearing and vision symptoms were suspected to be due to injury and edema in the tectum. After starting gabapentin, he reported increased tolerability of his tinnitus as the dose was increased, but no change in its intensity. He was seen by audiology and found to have bilateral mixed sensorineural and conduction hearing loss, worse on the right. After completing a dexamethasone taper, he noted worsened tinnitus so was treated with a longer prednisone taper. Communication improved with the use of a speech-to-text app, with adjustable text size and purposeful positioning to accommodate for his visual changes. On discharge his follow-up included oncology, radiation oncology, audiology, neurosurgery, and ophthalmology.
Discussion (relevance): Glioblastomas located in the pineal region are rare and it is uncommon to have a patient with tinnitus, hearing loss, cranial nerve IV palsies, and DMS. This also presented unique rehabilitation challenges as the patient had changes to his hearing and vision that affected communication throughout the stay.
Conclusions: A pineal region glioblastoma can present with an unusual constellation of symptoms leading to communication and rehabilitation challenges.

.jpg)
 photo")
