Resident Ohio State University Hospital PM&R Program Grove City, Ohio
Disclosure(s):
Nancy Tian, MD: No financial relationships to disclose
Case Diagnosis: Autonomic dysfunction in the setting of spinal cord injury (SCI) due to neurosarcoidosis.
Case Description or Program Description: While admitted for inpatient rehabilitation, a 65-year-old male with a non-traumatic C4 SCI, secondary to neurosarcoidosis developed episodes of orthostatic hypotension and sinus bradycardia. Infectious work up was negative and clinically symptoms were not indicative of autonomic dysreflexia. Cardiology determined his bradycardia was vagally mediated and no further work up was recommended. He was started on midodrine with improvement of hypotension, but his bradycardia persisted. During a Hoyer lift transfer, the patient arrested and required 3 rounds of ACLS before achieving ROSC and was emergently transferred to acute care.
Setting: Inpatient rehabilitation, with eventual transition to acute care hospitalization.
Assessment/Results: In acute care, he was placed on continuous cardiac monitoring. He continued to have brief episodes of sinus pauses, typically overnight. An echocardiogram was unremarkable. He again had an episode of asystole, requiring further rounds of ACLS. Given the multiple episodes of sinus pauses and asystole, cardiology proceeded with placement of a pacemaker.
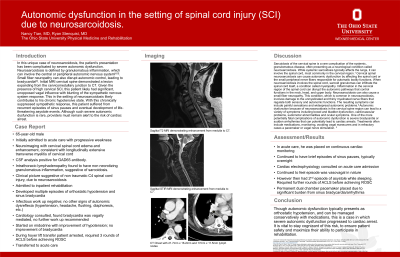
Discussion (relevance): This patient’s neurosarcoidosis was complicated by severe autonomic dysfunction. Initial MRI cervical spine demonstrated a lesion expanding from the cervicomedullary junction to C7. With a high cervical SCI, this patient likely had significant, unopposed vagal influence with blunting of the sympathetic nervous system response. This likely led to his chronic hypotensive state, recurrent episodes of sinus pauses, with eventual development of life-threatening asystole events. Although such severe autonomic dysfunction is rare, providers must remain alert to the risk of cardiac arrest.
Conclusions: Though autonomic dysfunction typically presents as orthostatic hypotension, and can be managed conservatively with medications, this is a case in which severe autonomic dysfunction progressed to cardiac arrest. It is vital to stay cognizant of this risk, to ensure patient safety and maximize their ability to participate in rehabilitation.

.jpg)