Physical Medicine and Rehabilitation Resident Ohio State University Hospital PM&R Program, Ohio
Disclosure(s):
Chad M. Burkholder, MD: No financial relationships to disclose
Case Diagnosis: A rare and interesting case of intrathecal methotrexate-induced spinal cord injury
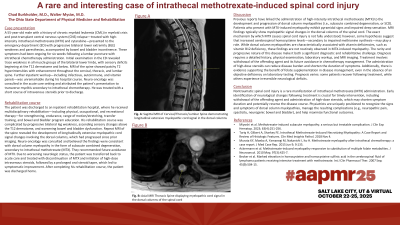
Case Description or Program Description: A 55-year-old male with history of CML myeloid crisis with post-transplant CNS relapse receiving intrathecal methotrexate and cytarabine presented with progressive lower limb weakness, paresthesia’s and mild bowel/bladder incontinence for 6 weeks following lumbar puncture with IT chemotherapy administration. Exam revealed trace weakness in bilateral lower limbs and sensory changes beginning at T12 and below. MRI showed patchy T2 hyperintensity and enhancement of the cervical, thoracic, and lumbar spine. Additional infectious, autoimmune, and vitamin panel workup unremarkable. Neuro-oncology believed current presentation secondary to transverse myelitis in setting of intrathecal chemotherapy. He received IV steroids and short oral steroid taper prior to discharge. He transferred to inpatient rehabilitation where he experienced progressive leg weakness, ascending sensory deficits and worsening neurogenic bowel/bladder. Repeat spine imaging revealed development of longitudinally extensive myelopathic cord signal involving the dorsal columns of the thoracic cord suggesting subacute combined degeneration. Repeat workup ruled out infectious, autoimmune or vitamin deficient etiologies. Neuro-oncology determined the worsening symptoms and imaging findings were due to progression of disease secondary to intrathecal methotrexate.
Setting: Inpatient rehabilitation
Assessment/Results: Treatment with high dose IV steroids and prolonged oral steroid taper was initiated with improvement.
Discussion (relevance): Previous data has linked the administration of intrathecal methotrexate to development of dorsal column myelopathy mimicking subacute combined degeneration. The infrequency and progression that is encountered makes it a formidable diagnostic and rehabilitative challenge. The diagnosis requires a detailed history, physical exam, laboratory workup and MRI imaging.
Conclusions: A nontraumatic spinal cord injury is a rare consequence of intrathecal chemotherapy in treatment of hematologic malignancies. Management of this condition includes steroids and withdrawal of the toxic agent. There is minimal research that identifies the benefit of folate supplementation in treatment of this disease.

.jpg)